ASA™ is a tool for early identification of young children who might be at risk for auditory skill deficits and/or early literacy skill difficulties. This screener provides accurate, developmentally based results to help determine which children may need follow-up, intervention, or further evaluation.

Auditory Skills Assessment
ASA
ASA™ is a tool for early identification of young children who might be at risk for auditory skill deficits and/or early literacy skill difficulties. This screener provides accurate, developmentally based results to help determine which children may need follow-up, intervention, or further evaluation.
- Age range:
- 3:6—6:11
- Publication date:
- 2010
- Qualification level:
- B
- Completion time:
- Completion Time: About 5 minutes (ages 3:6— 4:11); About 15 minutes (ages 5:0—6:11)
- Administration:
-
Paper-and-pencil/CD-ROM
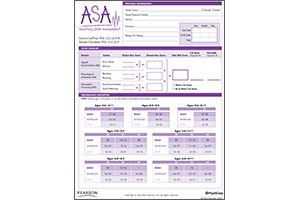
- Scores/Interpretation:
- Overall cut scores
- Scoring options:
- Manual scoring
Use ASA to screen children for early auditory and phonological skills, and get fast results to put children on the right track.
Benefits
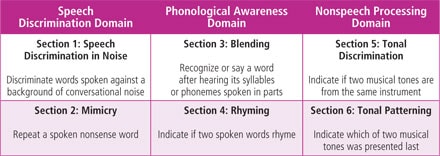
- Assesses auditory skills critical to the development of oral and written language skills.
- Serves as a low-tech, friendly screener for young children (no headphones or audiometer required).
- Indicates performance across each domain on the ASA, which may indicate a need for further follow-up evaluation, immediate intervention/instruction in auditory skills, or re-screening.
- Offers the youngest age range in a published auditory skills screening and can provide an early warning indicator.
- Reflects best practices in behaviorally based auditory screening.
- A perfect companion to routine hearing screenings within the given age range.
Features
The ASA is designed to be a quick, reliable indicator of a young child’s auditory skills and includes the following features:
- Unscored practice items provide opportunity to teach the tasks.
- Individual, untimed administration and scoring procedures that are quick, easy, and objective.
- No required reading or written responses.
- Large, full-color illustrations tested to appeal to young children.
- An indicator of performance (high, average, low) pinpoints further assessment or intervention needs.
- Case studies highlighted in the manual for supported use of the ASA.
- Standardized from December 2008 through May 2009; over 600 children were tested at 123 locations.
Resources
The following resources are available for Auditory Skills Assessment.
Questions and responses follow. Responses are from the test’s author.
Considering the various professional scopes of practice, the audiologist is best equipped to make the formal diagnosis of APD. However, in some districts there are no audiologists to do the testing and the SLP has the testing instruments to, at least, do screening. Under those circumstances, the SLP should complete an assessment and refer out to an audiologist for detailed testing if the SLP suspects APD. I suggest the SLP evaluate the child's listening comprehension skills, since a deficit in receptive language often looks like an APD. Further, since the SLP is the one who does the therapy, there is more than one role for the SLP, as usual. It is not an uncommon controversy—often I hear, "If the SLP does the therapy, why can't he or she diagnose the problem?" Again, this is a scope of practice and expertise issue. It would be best to work in tandem and have an audiologist consult in the assessment process, at a minimum. That said, I am not in favor of having a psychologist diagnose APD. I am familiar with their typical test instruments which can be used to classify APD, which looks at APD mainly from a processing standpoint of phonological skills. Diagnosing from that perspective alone is not always accurate. Again, working with the audiologist and the SLP will support the diagnostic process best.
As with any assessment of a student who is learning English as a second language, best practice that you choose a combination of formal and informal measures in the primary language and use a process of gathering data across the settings of the student's life. The ASA could be used informally (i.e., without scores) if appropriate, especially the non-linguistic tasks.
While oral language skills are "hard-wired" in the brain and typically developed through experience and the child's environment, written language skills must be taught. Phonological awareness tasks use oral language skills can be learned through oral language experience and practice. Some children learn sound awareness and manipulation skills easily in conversation and language play with others. However, many children need explicit instruction in phonological awareness as a precursor to written language instruction. In either case, the ASA can be used effectively even before direct instruction is given in phonological awareness.
The ASA is a screening tool, and therefore is not an assessment to be used for eligibility purposes. The goal is early screening—which answers the question of risk status for deficits in auditory/listening skills. Certainly, screening data should be considered in the overall assessment process. The value of the early assessment helps keep the child "on the radar" and potentially benefit from an early intervention process, perhaps as in a Response to Intervention model.
Page 11 in the ASA manual states, "If you determine that an articulation error affected a response that was otherwise correct, you should score the response as correct; do not penalize a child for articluation errors. If a child has severe articulation errors and is unintelligible, these sections should not be administered. Record a total section raw score of 0 and continue to the next section."
Of course! Experts in reading and/or language have key training to support the phonological system in the development of reading. Depending on your particular setting and workflow, either or both disciplines may support phonological skill development in a particular child.
The background noise for Speech Discriminiation in Noise is provided by the ASA on the Stimulus CD. The examiner should provide a distraction-free environment, in a quiet, well-lit room. The background noise on the Stimulus CD is a conversation-based cafeteria noise with a +6dB signal-to-noise ratio (SNR).
You might position the use of the ASA as part of your annual vision and hearing screening efforts. The ASA is a perfect companion to the hearing screening process.
Yes! You could choose to use the tasks from the ASA for older children descriptively. Of course, the normative data only go through 6:11.
You can. Keep in mind that if the delay is around articulation/phonology, you should follow the manual on scoring regarding these types of errors. Overall, children with speech and language delay were excluded from the normative sample because at this young age it would be difficult to discriminate language from auditory difficulties. See pages 11 and 24 in the manual regarding these two thoughts, respectively.
It depends on the age of the child. Younger children only complete Section 1: Speech Discrimination in Noise and Mimicry. Older children complete all six tasks.
A figure-ground deficit is the inability to block out background noise and focus listening to the foreground (i.e., the speaker).
Yes. If the child's cochlear implants are in good working order and the child passed a hearing acuity screening according to the specifications in the manual, the child may be administered the ASA descriptively.